Anterior shoulder dislocation: pre- and post-operative management of a stop
Article written by Antoine FRECHAUD and Nathan Touati, publishing directors at NeuroXtrain Who are we? Antoine Fréchaud and his partner Nathan Touati are at the
Article written by Antoine FRECHAUD and Nathan Touati, publishing directors at NeuroXtrain

Antoine Fréchaud and his partner Nathan Touati are at the head of NeuroXtrain, website specializing in writing articles and creating various content on sports sciences, performance, new technologies and athlete rehabilitation.
Anterior glenohumeral joint dislocations are the most frequently encountered joint dislocations. They can be the result of low or high energy trauma.
The spectrum of problems linked to shoulder instability extends from pain due to instability to complete dislocations. The natural history, treatment and prognosis differ depending on the diagnosis. Anterior glenohumeral (GH) dislocation is the first common presentation of shoulder instability encountered by clinicians. GH dislocations account for approximately 50 % of all joint dislocations, of which 95 to 97 % are anterior dislocations.
The inherent mobility of the GH joint comes at the expense of stability. Static and dynamic constraints ensure the stability of the GH. Static stabilizers include the glenoid labrum, glenohumeral ligaments, articular concavity of the glenoid fossa, and intra-articular pressure. Dynamic stabilizers include the rotator cuff muscles, periscapular muscles, and biceps tendon.

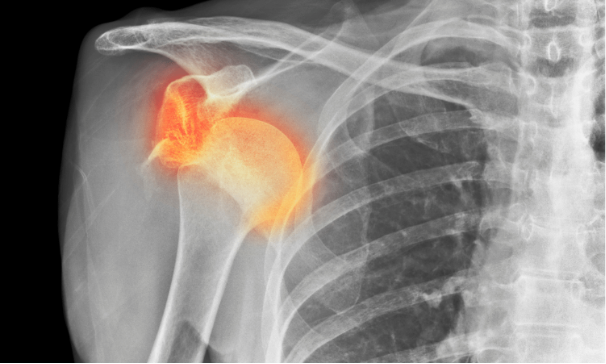
In an anterior dislocation, the arm is in a position of abduction and external rotation. In the external rotation position, the postero-superior face of the humeral head abuts and crosses the antero-inferior face of the glenoid border. This can damage the humeral head, the glenoid labrum, or both. An associated compression fracture of the humeral head is described as a Hill Sach injury. If severe enough, it can lead to locked dislocations that may require open reduction. The glenoid labrum is a fibrocartilaginous structure that surrounds the circumference of the glenoid fossa. Bankart lesions are lesions of the anteroinferior glenoid labrum complex and are the most common capsulolabral lesion. A “Bankart bone” lesion refers to an associated fracture of the glenoid rim. These capsulolabral lesions are risk factors for recurrent dislocation.
Acute management consists of reduction of the dislocation and immediate immobilization. The immobilization position remains a subject of debate. The duration of immobilization described also varies from one to six weeks. Studies comparing the method and duration of immobilization remain necessary.
Managing pain and local inflammation involves applying cold locally. Using cold helps control inflammation without completely interrupting it, unlike an anti-inflammatory medication. Inflammation is essential for healing, so it is necessary to regulate it rather than eliminate it completely. This avoids excess edema which could hamper the operation or post-operative rehabilitation. During this first phase, local application of cold is therefore the preferred method, combined with compression for optimal effectiveness. Cold and compression play a key role in recovery from tissue damage by reducing cellular metabolism, delaying nerve conduction, limiting edema expansion, and relieving pain.

One of the flagship products of the recovery range Orthonov, THE Cryopush, is a battery-powered portable device. It offers athletes the opportunity to take care of their body by improving their recovery process. The benefits of cryotherapy are widely recognized, whether for the post-injury phase, sports recovery or post-operative periods. With the Cryopush, it is possible to use the device on one or two areas simultaneously, in compression mode alone or by combining compression with a pre-cooled gel pack according to your specific needs. THE Cryopush, with its shoulder kit, proves to be the ideal device to solve these problems, whether in the case of previous dislocations or post-operatively for these injuries.
Long-term treatment plans are tailored to patients based on their age, activity level, and history of recurrent dislocation or chronic instability. In younger patients, surgical planning should be implemented, given the high rates of dislocation recurrence. Age is the main predictor of recurrence, with the highest rates seen in patients younger than 30 years old. Injuries such as Hill Sach's, Bankart and Bony Bankart are injuries associated with anterior shoulder dislocations. There is a prevalence of 73 % of concomitant Bankart lesions.
Greater than 20 % damage to the glenoid may be an indication for surgical evaluation. Recurrence rates are extremely varied, but can reach 70 %. Quantification of these bone lesions is important to dictate surgical management and reduce the risk of recurrence. In cases of isolated Bankart lesions, arthroscopic labral repairs offer satisfactory results. If the patient is younger or has more complex pathology, a simple arthroscopic procedure may not be as effective.
The Instability Severity Index score was developed to help guide treatment between an arthroscopic procedure and an open stabilization procedure. In cases of excessive bone damage, more extensive procedures are necessary. For severe injuries to the humeral head, the Filling procedure has been successful in reducing the number of dislocations. Filling means filling the humeral head defect with the posterior capsule and infraspinatus to prevent the humeral head from engaging in the glenoid. In cases of significant glenoid loss, coracoid transfer procedures, such as the Latarjet, prevent dislocations through multiple mechanisms. A transferred section of the coracoid process provides static stabilization by filling the bony defect and acting as a bone block. The conjoined tendon, which is transferred with the coracoid, has a sling effect providing dynamic stabilization. In elderly patients with rotator cuff tears, rotator cuff repair rather than reverse total shoulder arthroplasty should be considered depending on the patient's age, activity level, tissue quality, rotator cuff and pre-existing glenohumeral arthritis.
If nonoperative treatment is pursued, a rehabilitation protocol involves return to movement, dynamic stabilization, neuromuscular training, and strengthening. The initial phase may be devoted to symptomatic pain management and gentle range of motion. As range of motion is regained and pain subsides, attention can be shifted to active range of motion and strengthening. Subsequent stages of rehabilitation can then focus on advanced strengthening with a gradual return to activity through explosive and plyometric exercises.
Postoperative rehabilitation protocols balance soft tissue healing with prevention of postoperative stiffness. Most surgeons will place postoperative patients in immediate immobilization. The duration varies from one to six weeks. A typical postoperative protocol may involve a period of soft tissue rest to protect any repair. In conjunction with this delay, certain exercises with an amplitude and type of contractions under the supervision of a physiotherapist can be started. The goal is to return to pre-injury level. Comparing arthroscopic and open stabilization procedures, a 2017 systematic review found no differences in return-to-play rates and patient-reported outcomes. In all surgically treated patients, more than 65 % athletes returned to their pre-injury level of play.

Anterior shoulder dislocations are the most common joint dislocations. When patients present to the emergency room, appropriate x-rays are necessary for an accurate diagnosis. Patient education is important for patients with a history of one or more dislocations. Recurrent dislocations can lead to additional chondral damage, bone loss, and disruption of soft tissue stabilizers. Positions that put the joint at risk, including extreme abduction and external rotation, should be avoided. Younger patients and athletes should be informed of their particular risk of recurrence.
All content in this article is presented for informational purposes. It does not in any way replace the advice or visit of a health professional.
Sources:
Article written by Antoine FRECHAUD and Nathan Touati, publishing directors at NeuroXtrain Who are we? Antoine Fréchaud and his partner Nathan Touati are at the

Article written by Antoine FRECHAUD and Nathan Touati, publishing directors at NeuroXtrain Who are we? Antoine Fréchaud and his partner Nathan Touati are at the

Article written by Antoine FRECHAUD and Nathan Touati, publishing directors at NeuroXtrain Who are we? Antoine Fréchaud and his partner Nathan Touati are at the

Article written by Antoine FRECHAUD and Nathan Touati, publishing directors at NeuroXtrain Who are we? Antoine Fréchaud and his partner Nathan Touati are at the